
Patient stories are split across sources
The same systemic issue shows up differently depending on which part of the chart a clinician is reviewing. Encounters, notes, diagnoses, and orders live in separate modules—clinicians compare dates across tabs to rebuild chronology and lose surrounding context when any one view is opened in isolation.
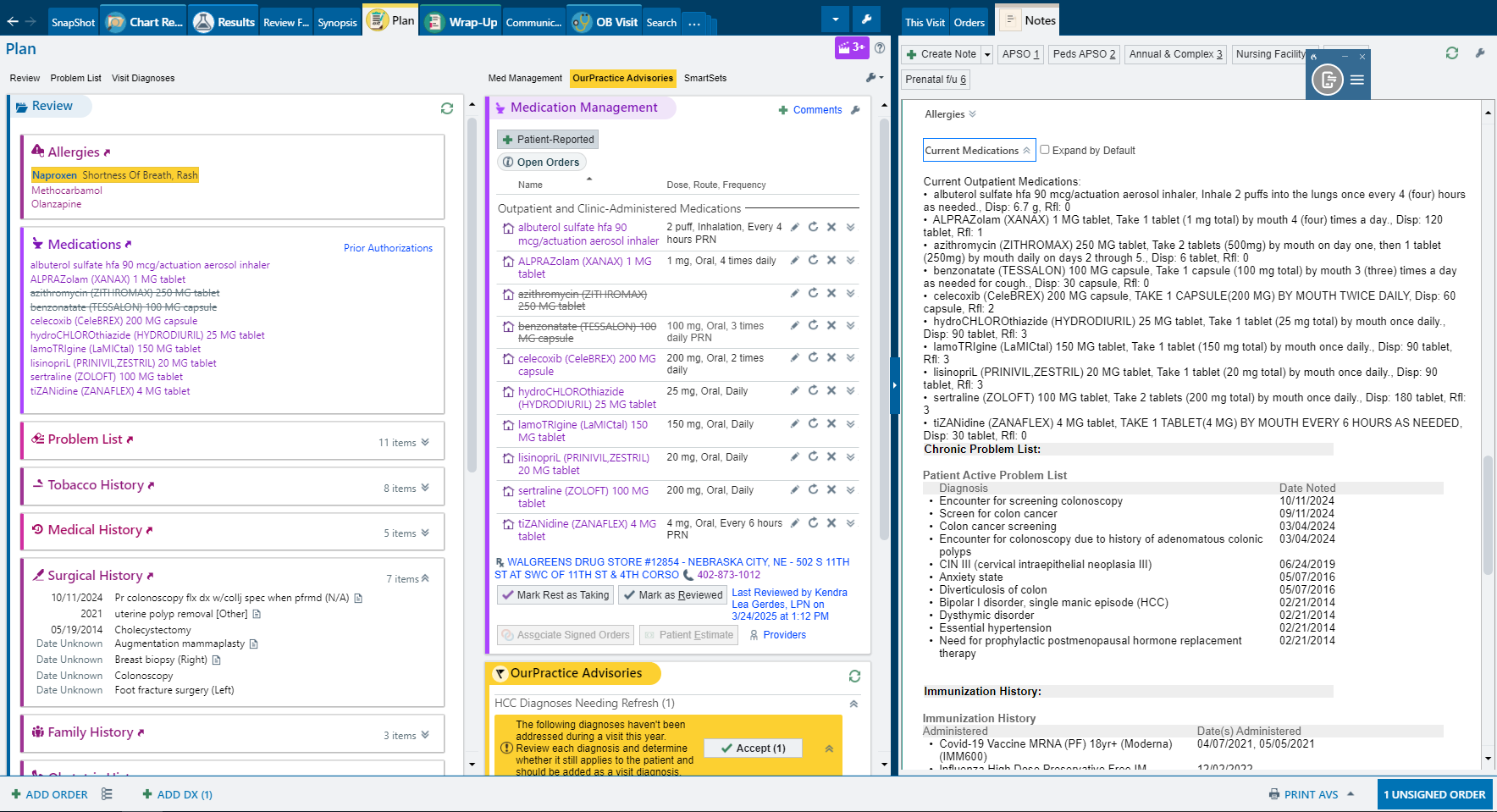
Encounter list: Events are chronological, but the longitudinal story still has to be assembled manually.
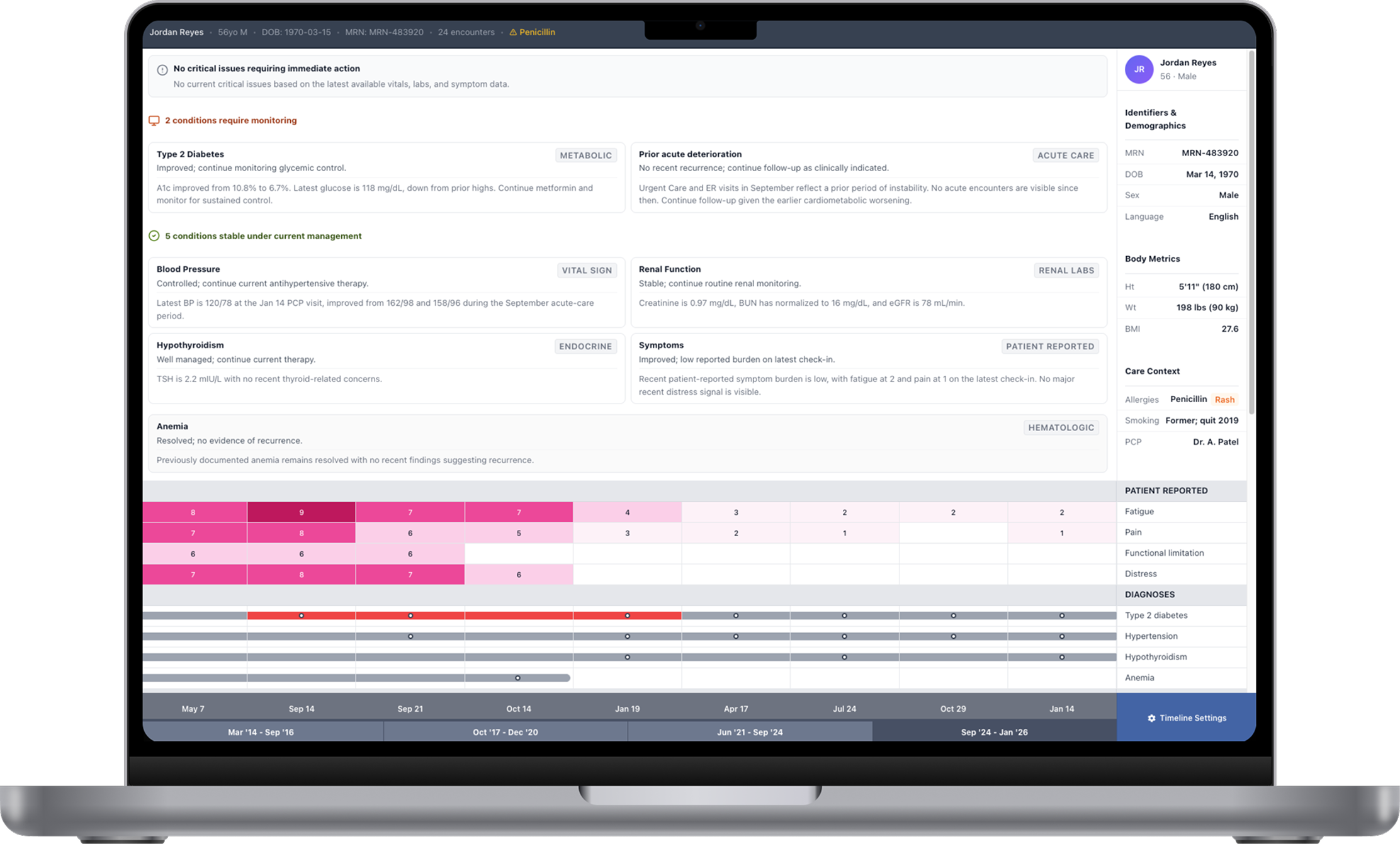
Visit report: Diagnoses and orders are visible, but disconnected from labs, medications, and symptoms at adjacent visits.