Reimagining problem list management with clinicians
In 2015, I worked with the DoD to research EHR usability. During a 2-week sprint, I co-designed approaches to problem list reconciliation with working physicians.
The problem
The Problem List is a Shared Pain Point
“Problem lists are the problem of all EMRs:
no one does a good job of presenting them.”
— Health informatics expert
It Becomes Overwhelmingly Large
As diagnoses accumulate over time, clinicians struggle to quickly identify the most relevant information. Critical context becomes buried in long, difficult-to-scan records.
It Becomes Redundant
Inconsistent documentation practices often lead to duplicate or overlapping diagnoses, creating unnecessary noise and reducing trust in the data.
It Lacks Clear Governance
Clinicians disagreed on what belongs in the problem list, revealing the absence of shared standards for maintaining meaningful and clinically useful records.
Prototyping
Fast, Direct Reconciliation
“Something that lets you somehow update the problem list in a user-friendly way that takes like five seconds.”
— Emergency physician
Direct manipulation
Early concepts supported the right relationships, but they asked for too much navigation—new windows, extra taps, and heavy attention shifts.
Letting clinicians drag one problem onto another to define a relationship became the core of the interaction: fewer steps, less context switching, more time on the clinical decision.
Hick's Law
Too many relationship types slowed people down. I collapsed the set to two high-value options: Similar to for duplicates and close cousins, and Secondary to when one problem was a consequence or symptom of another.
Click-through prototype: Shown to clinical SMEs for qualitative feedback on speed and clarity.
Refinement
Status, Timing, and History
“We sometimes see quiescent inflammation that becomes active, then back to quiescent and back to active.”
— Ophthalmologist
When was it last active?
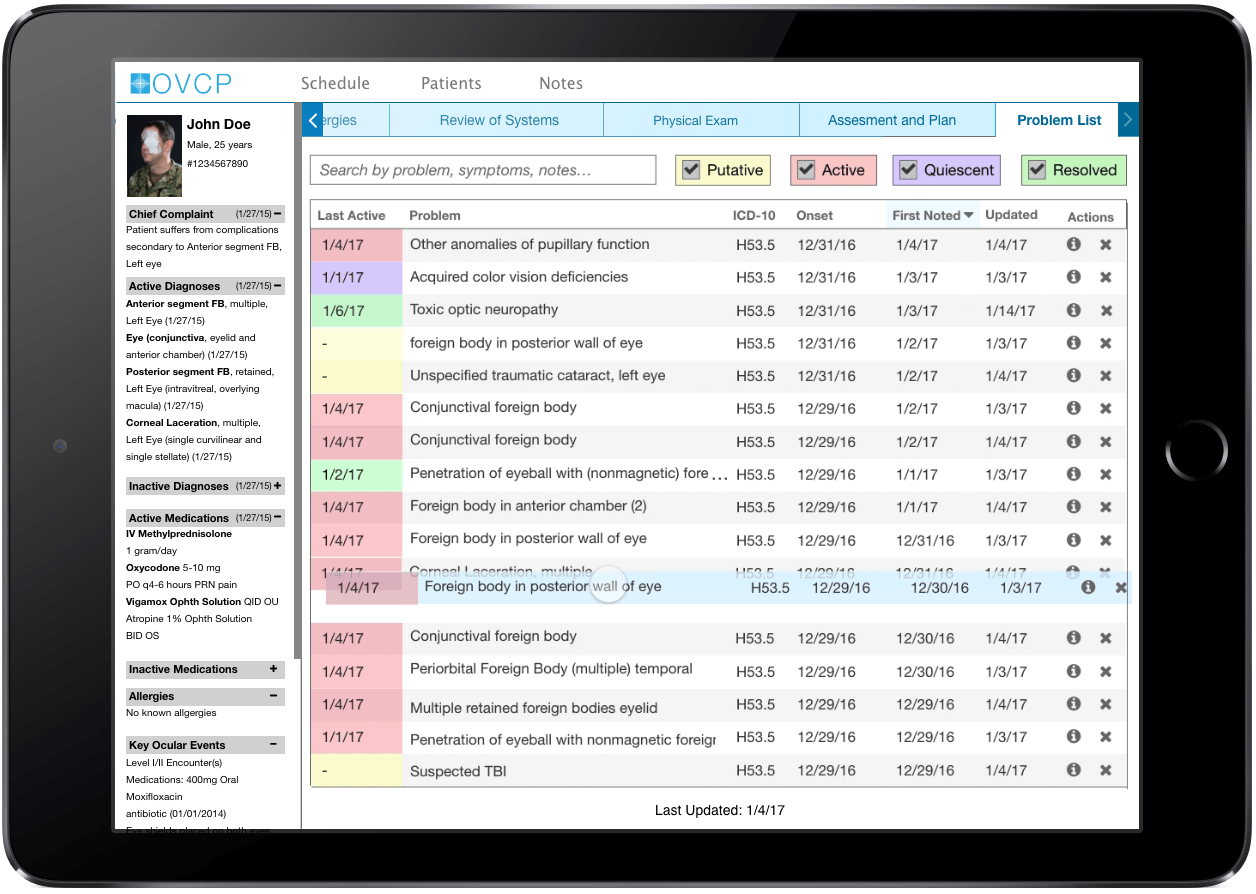
Recurrence timing often signals when management should change. I explored sort orders that surface last active alongside status tags (putative, active, quiescent, resolved) so the list reads as a timeline, not just a stack of labels.
What's the history of the problem?
An info view could expose the full arc for a diagnosis—labs, referrals, notes—scrubbed through a compact activity strip so clinicians could see quiet and busy periods at a glance.
Linking common workups to a diagnosis could also reduce missed follow-up when the chart is dense.
Later iteration: Resolved filters, info affordances, and calmer hierarchy for review.
Formative feedback
What Clinicians Said
Qualitative sessions validated the direction; together with structured feedback, the program advanced toward summative testing.
This is an efficient and effective method for problem list reconciliation.
- 60% strongly agreed
- 40% agreed
- 0% were neutral or disagreed
“I like the tools used to better represent the clinical picture.”
This novel method of reconciling the problem list will support more effective care coordination.
- 80% strongly agreed
- 20% were neutral
- 0% disagreed
“This is a great way to provide a sub-structure to the overall list, a great feature to reduce clutter.”